Cranial Cruciate Ligament Injuries
Inside the knee there are two ligaments that control relative movement between the femur and the tibia. They cross each other and thus are called the cruciate ligaments. One is called the caudal cruciate ligament. The other is called the cranial cruciate ligament (CCL). In humans this is called the anterior cruciate ligament
(ACL). In both species, the latter (CCL/ACL) is prone to partial and full rupture. After partial and/or full rupture of the CCL the excessive motion and strain between the femur and the tibia leads to pain, cartilage damage, and eventual arthritis.
Dogs with a CCL tear or partial tear usually will not bear weight with the affected leg. Surgery is required to correct the condition. Multiple studies repeatedly show that in the immediate term (initial days to weeks) and long term (months to years) dogs do significantly better with repair versus non surgical (medical management). The modes of assessment that show that surgery produces better outcomes are force plate analysis (measures amount of load that the dog puts on the legs), owner perception, and veterinarian perception. The force plate analysis is a very objective measure, and the owner and veterinarian perceptions give a good measure of functional use.
The two primary repair options are the Tibial Plateau Leveling Osteotomy (TPLO) and the Tibial Tuberosity Advancement (TTA).
Tibial Plateau Leveling Osteotomy (TPLO) in San Diego- current price $2600 patients approximately 40-89 lbs (inquire regarding other weight ranges)
The TPLO corrects the torn/partially torn CCL by re-orienting the tibial plateau (the top of the tibia) so that it is more nearly flat. This eliminates excessive fore and aft force and motion of the femur relative to the tibia, termed cranial thrust. The simplest model that explains this well is the wagon on the hill example. Imagine a wagon (the femur) connected to a post on a hill (the tibial plateau) by a rope (the CCL).
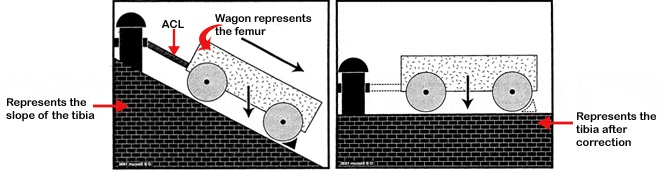
As the angle of the hill increases, the greater the load on the rope (CCL). The theory is that this excessive tension plus a collagen defect in the ligament leads to rupture or partial rupture. The angle of the hill is the tibial plateau angle and if this angle is eliminated (or nearly eliminated) the excessive force on the rope (CCL) and other critical parts of the knee (e.g. meniscus) joint is eliminated or greatly reduced.
The TPLO procedure essentially flattens the tibial plateau angle to eliminate these damaging forces in the knee. As you can see in the radiographs, the tibial plateau angle after surgery is nearly horizontal, compared to the significant slope prior to surgery. The TPLO does not replace or approximate the damaged CCL, but it drastically reduces the need for it by correcting the tibial plateau angle.
Tibial Tuberosity Advancement (TTA)
The TTA corrects the torn/partially torn CCL by changing the direction at which the quadriceps (thigh muscles) pull. The pull of the quadriceps not only straightens the knee, but it also tends to pull the tibia forward (cranial thrust). Studies have shown that if this pull is directed at 90 degrees to the tibial plateau then the tendency to pull the tibia forward is eliminated. The TTA accomplishes this by moving the attachment point of the quadriceps tendon on the tibia forward.
TPLO vs TTA
Both of these surgeries produce excellent outcomes and have situations where one may be preferred over the other. However there is no consensus of data or consensus among surgeons as to whether the TPLO or the TTA is inherently superior. That being said, there may be particular situations in which one may be better suited to correct concurrent problems (i.e. luxating patella, femoral bow, etc). As such, each case we assess individually, and working with you, select the most appropriate procedure based on your individual pet, your goals, concurrent orthopedic conditions, and other concurrent conditions.
Recovery and Rehabilitation
Every case is unique, but most of the dogs with a cruciate repair walk out of the hospital the same day of surgery. A limp will be present but, some are toe touching. The patients gradually use the surgical leg more and more as time goes on. It is your responsibility however, to eliminate excessive use. We supply specific and detailed week by week recovery and rehabilitation instructions. A main point of these is that no off leash activity, and no running, jumping, rough playing is allowed until 16 weeks after surgery. If at any point there are questions or concerns, we can be reached via a phone call or email and are very responsive to resolving your concerns, as we are fully aware that good outcomes have a lot to do with attentive follow up.
AAHA Accredited Hospital
Being an AAHA Accredited hospital, you can have comfort knowing that your pet will be receiving the highest standard of care. We have demonstrated a commitment to this high level of care through adherence to the standards and passing periodic, comprehensive, third party on site and off site evaluations. Only 12-15% of veterinary hospitals in the US and Canada are accredited by AAHA, so we are very proud of this, and we know that it makes a difference in the overall quality of care that we provide to your pet, surgery included. For more details about the benefits of doing your procedure in an AAHA certified hospital, see the AAHA webpage.
In summary, we promise to communicate with you throughout the process, and make your pet's surgery as stress-free, pain free, and beneficial as possible.
If you have any questions or comments about how we can help your pet through orthopedic surgery, please contact us today for a complimentary orthopedic exam. You may call us, email us, request more information, or directly request a complimentary orthopedic exam.


